

Translate this page into:
Infant and Young Child Feeding Behaviors among Working Mothers in India: Implications for Global Health Policy and Practice
Abstract
Background:
The National Guidelines on Infant and Young Child Feeding introduced in 2006 recommended the initiation of breastfeeding immediately after birth, preferably within one hour; exclusive breastfeeding for the first six months; appropriate and adequate complementary feeding from six months of age while continuing breastfeeding; and continued breastfeeding up to the age of two years or beyond. Working women in India constitute a dominant and expanding pool of mothers. There is paucity of research focused on feeding behavior within this group.
Method:
One hundred and fifty working women answered a structured questionnaire about their demographics, birth history, levels of awareness and practice of feeding guidelines, and perceptions about breastfeeding and counseling. Data analysis was carried out using Microsoft Excel and the Statistical Package for the Social Sciences.
Results:
Majority of participants belonged to 21-39 years age group, had nuclear families, received college education, and delivered in institutional setups. Gaps were observed between the mother's levels of awareness and practice for different tenets of national guidelines. Higher education, longer maternity leave, higher income, and utilization of counseling services facilitated adoption of optimal feeding behavior. Most women perceived breast milk to be superior to any alternative and favored provision of counseling during last trimester.
Conclusions and Global Health Implications:
Counseling women on optimal feeding behavior is a potential intervention to convert its awareness into actual practice. The lessons learned from this study can help refine both national and global Mother and Child Health policies and programs.
Keywords
Breastfeeding
India
National
Guidelines
on
Infant
and
Young
Child
Feeding
Working
mothers

Introduction
Optimal nutrition during first two years of life is crucial for the survival, healthy growth, and development of infants and young children.[1] Ensuring optimal breastfeeding for all children in the first two years of life has the potential to save lives of at least 800,000 under 5 children every year.[2] Optimal feeding of infants and young children, a crucial component of the Mother and Child Health, is as much a basic right of infants and young children as it is for their mothers since the latter are the only natural source of nutrition for the former.[3] The global status of the Mother and Child Health indicates that several countries including India have not been able to perform as anticipated. India ranks close to the bottom amongst countries with deficient performance on this front. This deficiency has been attributed to low levels of awareness and practice of optimal feeding practices among its women. As a result, India continues to lose millions of young lives year after year.[4] This is evidenced by the finding that in 2012, India recorded an Infant Mortality Rate (IMR) of 44 and the Under 5 Mortality Rate (U-5 MR) of 58 against the global averages of 35 and 48 respec- tively[5,6]
The Government of India issued National Guidelines on Infant and Young Child Feeding (NGIYCF) in 2006. Various studies and surveys indicate that such measures have failed to bring about the desired positive change. In India, 129.1 million strong group of working women comprises one of the most prominent and expanding community of mothers.[7] The feeding behavior of this group has remained an overlooked area of research till date.
Feeding behavior of a working woman is a combination of her perceptions, awareness, facilities, and support. It is more challenging for employed women to equilibrate their feeding responsibilities and work. The positive impact of early initiation and exclusive breastfeeding for the first six months has been clearly demonstrated to prevent nearly one- fifth of neonatal deaths whereas a delay of just one day has been shown to advance the death rate by 2.6 times.[8] They also demonstrated that in fully breastfed infants, the first month infection-related death risk was just one third the risk observed in partially breastfed infants. It is known that working full time has a strong negative impact on duration of breast-feeding.[9]
Employment modifies breastfeeding behavior of a woman in significant manner with full time employment having the most detrimental impact.[10-12] Mandal and his co-workers established that in comparison with non-working mothers, probability of breastfeeding cessation among full time workers was four times as high for women availing a maternity leave of less than six weeks while it was just half as much for women with less than 12 weeks of leave.[13]
Studies on women from different parts of India substantiate widespread prevalence of suboptimal feeding practices. A study from Northern India reported that breastfeeding within one hour and exclusive breastfeeding for six months was practiced by only 19% and 5% women respectively.[14] Several studies from the Western and Eastern India confirm significant lapses in the feeding behavior of mothers. [15-20] As a consequence of suboptimal feeding behavior among mothers, India is struggling to achieve the targeted reduction in the U5-MR by two-thirds between 1990 and 2015 as stipulated under MDG-4 while failing to meet its own targets as well. It is apprehended that India will attain MDG-4 targets at least a decade behind schedule.[21]
Being the capital city of India, New Delhi is home to working women from all parts of country and with heterogeneous characteristics. This study focused on working women in the organized sector to explore their levels of awareness and practice of NGIYCF. It also attempts to find a solution to the problem at hand. The findings of this study have the potential to be extrapolated for greater understanding of breastfeeding attitudes of working women in other metro cities as well, both within and outside India. The lessons drawn from this study can be utilized to fine-tune the Mother and Child Health policies and programs at a global scale.
Methods
Setting.
The present study was conducted in New Delhi between October 15, 2011 and February 20, 2012. The participants included 150 working women residing in Delhi, with each woman having an infant or young child between the ages of six months and two years. The study was approved by the Ethics Committee of Jaipur Golden Hospital, Delhi. The participants were approached while visiting physician's offices. We expected that most of the eligible women would approach physicians either for their personal or the infant or young child's regular check-up, immunization, or other ailments. Only married women were included who had delivered single baby at the last childbirth and were medically fit to breastfeed. Every participant was briefed about the method and scope of study. A verbal consent was obtained and no personal or identifying information was recorded. Data sheets were numbered and stored securely.
Data Collection.
Responses were recorded by participants on a 30- item structured questionnaire prepared by professionals from different fields. The questions related to information pertaining to their socio-demographic profile, birth history, awareness and practice levels of national guidelines, and perceptions about breastfeeding and counseling. Every participant was provided assistance in the form of a standby female healthcare provider. At the end of exercise, each participant was counseled about correct technique of infant feeding.
Statistical Analysis.
Data analysis was carried out using Microsoft Excel and the Statistical Package for the Social Sciences. Statistical analysis was performed using steps of cross tabulation, correlation of key variables with age, education, economic status, type of employment, type of family, type of delivery, gender of newborn, utilization of maternity leave, and utilization of pre-delivery and post-delivery counseling. The correlation coefficients thus obtained were finally tested for significance using t-test using standard formula. A p-value of 0.05 was taken as significant.
Results
Awareness of National Guidelines.
A significant gap was observed between awareness and practice levels of NGIYCF among the participants. At the time of delivery, 62% or 93 women and 82% or 123 women respectively were aware that breastfeeding should commence immediately after birth, preferably within one hour, and that exclusive breastfeeding is recommended for first six months. Furthermore, 69% or 104 women were aware that complementary feeding should be introduced after six months of age whereas 72% or 108 women were aware that breastfeeding along with complementary feeding is to be continued at least up to the age of two years or beyond.
Practice of National Guidelines.
We observed that initiation of breastfeeding within first hour was practiced by 54% or 81women and exclusive breastfeeding for six months was practiced by 38% or 57 women. Of the participants who did not complete exclusive breastfeeding for the recommended first six months, those completing exclusive breastfeeding for one, two, three, four, and five completed months was 11% or 10 women, 26% or 24 women, 42% or 39 women, 17% or 16 women, and 4% or 4 women respectively. Figure 1 shows the gaps between awareness and practice levels of different tenets of NGIYCF. We observed a sharp fall in the number of women practicing breastfeeding after three months. This event coincided with the initiation of complementary feeding. Initiation of complementary feeding before six months was practiced by 61% or 91 women while breastfeeding along with complementary feeding up to the age of two years was practiced by 70% or 105 women.
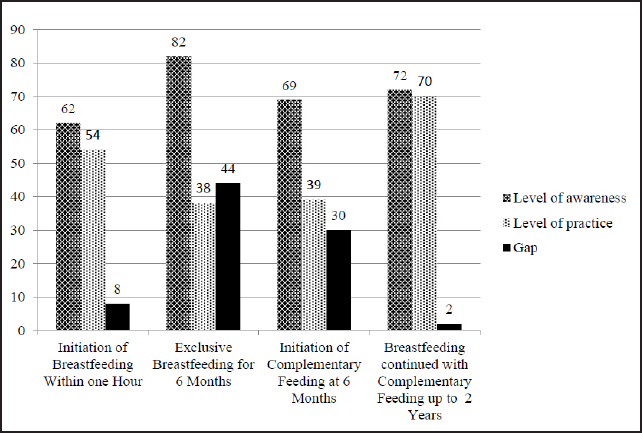
- Comparison of levels of awareness and practice, and their gap in relation to national guidelines
Impact of Education, Income, and Counseling.
College education and a higher family income level showed positive influence on compliance with national guidelines. It was further observed that counseling also had a similar effect.
Maternal Perceptions.
98% or 147 women perceived breast milk to be superior to any alternative. Counseling on optimal feeding behavior was favored by 99% or 148 women, with 63% or 94 of such women favoring counseling during last trimester of pregnancy.
We noticed that certain participant characteristics can be clubbed in order to identify potential groups of working women for future studies and interventions. Table 1 shows that most dominant group of women shared characteristics like age range from 21 and 30 years (77% or 116 women), graduation level education (83% or 140 women), employment in private sector (66% or 99 women), nuclear families (63% or 95 women), utilization of maternity leave (93% or 140 women), and monthly family income above 60,000 Indian Rupees or 1,000 USD approximately (55% or 83 women).
| Age of infant/young child (in months) | Number of cases (n=150) | Percentage |
|---|---|---|
| 6-7 | 7 | 5% |
| 7-8 | 11 | 7% |
| 8-9 | 8 | 5% |
| 9-10 | 10 | 7% |
| 10-11 | 27 | 18% |
| 11-12 | 11 | 7% |
| 12-15 | 18 | 12% |
| 15-18 | 23 | 15% |
| 18-21 | 16 | 11% |
| 21-24 | 19 | 13% |
| Place of delivery | ||
| Home | Nil | Nil |
| Hospital | 150 | 100% |
| Type of delivery | ||
| Normal | 64 | 43% |
| Caesarian | 86 | 57% |
| Birth order | ||
| First | 112 | 75% |
| Second | 35 | 23% |
| Third | 2 | 1% |
| Fourth | 1 | 1% |
| Gender of infant/ young child | ||
| Male | 87 | 58% |
| Female | 63 | 42% |
| Whether woman availed maternity leave | ||
| Yes | 140 | 93% |
| No | 10 | 7% |
| Duration of maternity leave (n=140) | ||
| Up to 90 days | 69 | 49% |
| Between 91-180 days | 71 | 51% |
| Whether woman received pre-delivery counseling | ||
| Yes | 65 | 43% |
| No | 85 | 57% |
| Whether woman received post-delivery counseling | ||
| Yes | 101 | 67% |
| No | 49 | 33% |
Discussion
The threat to lives of millions of infants and young children in India is a major national and global concern. It is ironic that most such deaths result from preventable causes. Various studies validate widespread practice of suboptimal feeding behavior among Indian women.[15-20] Working women constitute a significant and expanding pool of mothers in India whose feeding behavior has not been researched adequately. Therefore, there is a need to study levels of awareness and practice of recommended feeding behavior in this community.
Significant gaps between awareness and practice of national guidelines have been reported in Indian mothers from general population.[14,19] Our findings confirm existence of such gaps for different tenets of national guidelines among working women of New Delhi (Figure 1). The sharp decline in breastfeeding rates observed between third and fourth months signifies end of maternity leave for some women signaling their compulsion to return to work. Various studies have established that exclusive breastfeeding rates tend to be higher in women with a longer maternity leave or those not returning to work.[9,11,22,23] Ryan and co-researchers demonstrated that breastfeeding rates in the immediate post delivery period among part-time and full time working women were closer at 68.8% and 65.5% respectively; but the same rates diverged to 36.6% and 26.1% at six months.[11] Non-working women have been observed to outperform full time workers in breastfeeding.[24,25] End of maternity leave, therefore, is a crucial juncture in the feeding behavior of working women as it induces contemplation of alternate breastfeeding options including introduction of complementary feeding before the recommended stage.
We found that working women showed a universal preference for institutional deliveries. This signifies improved awareness about safe delivery among them. This preference offers an additional advantage in the form of an opportunity to women for closer interaction with healthcare personnel first to receive counseling and later to practice the same under their supervision. A motivated woman, enthused by her personal successful experience is more likely to repeat the behavior at subsequent childbirths. At the same time, it might turn her into a motivator and to counsel other women.
As shown in Table 2, there is a significant positive correlation between higher education and better compliance of optimal feeding behavior, a fact that is supported by several studies.[13,14,23,24] Conversely, several workers have reported lack of education as a significant barrier to optimal feeding behavior.[11,14,23]
| Participant Characteristics | Correlation co-efficient | t-test | p-value |
|---|---|---|---|
| Age | |||
| Awareness about EBF | -0.18 | -2.28 | 0.02 |
| Awareness about CF | -0.25 | -3.13 | 0.00 |
| Awareness about timing of introduction of CF after six months | -0.22 | -2.78 | 0.01 |
| Awareness that CF is to be continued along with BF up to 2 years | -0.17 | -2.05 | 0.04 |
| Perception about superiority of breast milk | -0.16 | -2.03 | 0.04 |
| Higher educational status | |||
| Awareness that BF should be initiated within first hour | -0.27 | -3.39 | 0.00 |
| Awareness about CF | -0.34 | -4.42 | 0.00 |
| Awareness about timing of introduction of CF after six months | -0.35 | -4.50 | 0.00 |
| Awareness that CF is to be continued along with BF up to 2 years | -0.29 | -3.72 | 0.00 |
| Higher economic status | |||
| Practice of EBF for six months | -0.23 | 2.56 | 0.01 |
| Practice of introduction of CF after six months | 0.25 | 3.12 | 0.00 |
| Utilization of pre-delivery counseling | |||
| Awareness that BF should be initiated within first hour | 0.64 | 10.10 | 0.00 |
| Awareness about EBF | 0.49 | 6.93 | 0.00 |
| Awareness about purpose of maternity leave | 0.35 | 4.48 | 0.00 |
| Awareness about CF | 0.56 | 8.23 | 0.00 |
| Awareness about timing of introduction of CF after six months | 0.57 | 8.44 | 0.00 |
| Awareness that CF is to be continued along with BF up to 2 years | 0.46 | 6.36 | 0.00 |
| Practice of initiating BF within first hour | 0.34 | 4.37 | 0.00 |
| Practice of EBF for six months | 0.16 | 2.02 | 0.02 |
| Practice of introduction of CF after six months | 0.23 | 2.86 | 0.00 |
| Utilization of post-delivery counseling | |||
| Awareness that BF should be initiated within first hour | 0.63 | 9.77 | 0.00 |
| Awareness about EBF | 0.59 | 8.93 | 0.00 |
| Awareness about purpose of maternity leave | 0.52 | 7.50 | 0.00 |
| Awareness about CF | 0.55 | 8.10 | 0.00 |
| Awareness about timing of introduction of CF after six months | 0.54 | 7.82 | 0.00 |
| Awareness that CF is to be continued along with BF up to 2 years | 0.39 | 5.13 | 0.00 |
| Practice of initiating BF within first hour | 0.35 | 4.54 | 0.00 |
| Practice of EBF for six months | 0.16 | 2.03 | 0.04 |
| Practice of introduction of CF after six months | 0.38 | 5.02 | 0.00 |
BF: Breastfeeding; EBF: Exclusive Breastfeeding; CF: Complementary Feeding
Counseling exerts a positive impact on the practice of optimal feeding behavior whereas its lack has an opposite effect.[14,26-28] The present study confirms the positive impact of counseling on such behavior. This view is further reaffirmed by the participants' perception as most of them concurred on the effectiveness of counseling. Most participants further suggested that counseling is likely to be most effective if provided during the last trimester of pregnancy. It is pertinent to point out here that an additional advantage of timely counseling would lie in its inherent potential to caution working women against the questionable influence of profit driven interests of formula feed manufacturers.
Both the age and higher educational status showed significant positive correlation with greater awareness of optimal feeding behavior. However, this relationship did not extend to better compliance in the practice of recommended behavior. This finding can be attributed to compulsion of working women to yield to the pressure of work despite being aware about fallouts of such a move. Thus, pressure to return to work seems to dominate feeding decisions of working women. We found that determinants like the employment sector of the woman, the type of delivery, and the gender of the infant did not influence feeding behavior significantly.
Although decision to breastfeed and adopt a suitable feeding behavior is a matter of personal choice for each working mother, yet it is prone to the influence of her peculiar circumstances. A lack of appropriate information and support from family, workplace, and society reduces the probability that a working woman would practice such reco- mmendations.[29] Thus, a breastfeeding friendly environment goes a long way in facilitating successful practice of optimal feeding behavior. In order to improve the Mother and Child Health status in India, there is a pressing need to strengthen programs and policies governing feeding behavior of mothers. It is imperative that the Indian government raises a work force of trained counselors to reach every eligible woman in the country. Such measures need to be bolstered by the government policies, womens' groups, media, employers, and healthcare providers. Unless such measures are instituted with urgency, employment will continue to take its toll on the health and lives of not only working women but also their infants or young children. Some researchers have proposed a reduction in working hours to facilitate optimal feeding behavior but the potential of such a measure remains to be explored.[11]
The core of participants in our study formed a distinct group on the basis of their age, educational status, employment characteristics, family structure, and level of income. Future research on working women can be aimed at different target groups so that existing policies, interventions, policies governing maternity benefits, and workplace facilities are aligned to the needs of these groups. We noticed that women availing six months maternity leave performed best in adopting optimal feeding practices. Therefore, we concur with Baker that a maternity leave of six months for all eligible women should be made a basic provision for successful implementation of guidelines on infant and young child feeding.[30]
The study calls for strengthening of counseling services in addition to uniform maternity leave of six months for all working women. For India, already struggling to bridge the gap between awareness and practice of national guidelines among its working women, there is nothing to lose but plenty of scope to improve its performance on Mother and Child Health programs by adopting such measures.
Conclusion
To our knowledge, this is the first study on feeding behavior involving working women in New Delhi. Our results confirm that the challenge of juggling between their feeding responsibilities and work is mainly responsible for working women's deviation from optimal feeding behavior. Counseling has the potential to improve feeding practices of such women and thereby move India closer to attaining its objectives pertaining to Mother and Child Health. A holistic approach is the need of the hour to attain this objective. Therefore, measures like setting up of a national counseling service by the Government of India to promote optimal feeding behavior as envisaged in the national guidelines and a six month paid maternity leave for all eligible working women are highly recommended. This study forms a foundational framework by analyzing feeding behavior of working women from the organized sector. However, there is a need to study feeding behavior of working women from the unorganized sector in order to gain a deeper understanding of the subject.
Global Health Implications
India is losing millions of young lives due to preventable causes. In India, the national guidelines on infant and young child feeding were issued in 2006. However, there is a clear gap between the awareness and practice of these guidelines. It is possible to bridge this gap with appropriate and timely counseling and creation of breastfeeding friendly environment. Lessons drawn from interventions on working women from India, therefore, can be utilized to devise and revise programs and policies being followed by countries struggling with high morbidity and mortality among their infants and young children. New Delhi shares a demographic similarity with several other metro cities within and outside India; therefore, it is possible to extrapolate results from the present study to understand and improve the situation in such places. We subscribe to the view that irrespective of geographical location, the needs of both the mothers and their infants or young children are identical as such needs are basic to human life and existence. The lessons drawn from the present study in conjunction with others have the potential to save millions of infants and young children worldwide that are prone to untimely and preventable deaths.
Financial Disclosure:
None.
Acknowledgements:
We would like to thank participants for their time and cooperation. We are highly grateful to Prof. Rachel Reimer of Des Moines University, Iowa, USA for her guidance. Our special thanks are due to fellow physicians Dr. Kanwal Kathuria, Dr. Praveen Kumar, Dr. Sonia Midha, Dr. Munish Kumar Midha, Dr. Shailesh Sharma, Dr. Sumedha Harne, and Dr. Manish Gupta for their help in data collection and valuable suggestions. We are deeply indebted to Dr. Arun Gupta for his encouragement and help.
Conflicts of Interest:
No authors have financial interests that pose a conflict of interest.
Funding Support:
None.
References
- Infant and young child feeding. Geneva: WHO; 2014. [updated 2014 February]. Available at: http://www. who.int/mediacentre/factsheets/fs342/en/ (accessed )
- [Google Scholar]
- Infant and young child feeding: Fact sheet N°342. Geneva: WHO; 2014. Available at: http://www.who.int/mediacentre/factsheets/fs342/en/ (accessed )
- [Google Scholar]
- van Leer Foundation. Implementing child rights in early childhood. The Hague: Bernard van Leer Foundation; 2006.
- [Google Scholar]
- What works? Interventions for maternal and child undernutrition and survival. Lancet. 2008;371(9610):417-40.
- [CrossRef] [PubMed] [Google Scholar]
- Global Health Observatory. Infant mortality. Situation and trends. [Internet] 2014 Available at: http://www.who.int/gho/child_ health/mortality/neonatal_infant_text/en/ (accessed )
- [Google Scholar]
- World Health Organisation. Global Health Observatory. Under-five mortality Situation: WHO, Geneva 2014 Available at: http://www. who.int/gho/child_health/mortality/mortality_ under_five_text/en/ (accessed )
- [Google Scholar]
- ILO Asia-Pacific Research Brief Series No. 2. A return to stronger employment growth in India? Insights from the 68th NSS Round 2011-12. Internatio nal Labour Organization Available at: http://www.ilo.org/wcmsp5/groups/public/---asia/---ro-bangkok/---sro-new_delhi/documents/genericdocument/wcms_228935.pdf (accessed )
- [Google Scholar]
- Breastfeeding and complementary feeding as a public health intervention for child survival in India. Indian Journal of Pediatrics. 2010;77(4):413-18.
- [CrossRef] [PubMed] [Google Scholar]
- The effect of work status on initiation and duration of breastfeeding. American Journal of Public Health. 1998;88(7):1042-46.
- [CrossRef] [PubMed] [Google Scholar]
- Through the magnifying glass: women's work and labor force participation in urban Delhi. Economic and Political Weekly. 2009;44(48):59-66.
- [Google Scholar]
- The effect of employment status on breastfeeding in the United States. Women's Health Issues. 2006;16(5):243-51.
- [CrossRef] [PubMed] [Google Scholar]
- On-the-job moms: work and breastfeeding initiation and duration for a sample of low-income women. Maternal and Child Health Journal. 2006;10(1):19-26.
- [CrossRef] [PubMed] [Google Scholar]
- The differential effects of full-time and part-time work status on breastfeeding. Health Policy. 2010;97(1):79-86.
- [CrossRef] [PubMed] [Google Scholar]
- Breastfeeding knowledge and practices amongst mothers in a rural population of North India: a community-based study. Journal of Tropical Pediatrics. 2009;55(3):183-88.
- [CrossRef] [PubMed] [Google Scholar]
- Breast feeding practices and health-seeking behavior for neonatal sickness in a rural community. Journal of Tropical Pediatrics. 2005;51(6):366-76.
- [CrossRef] [PubMed] [Google Scholar]
- Infant rearing practices and beliefs in rural inhabitants of Himachal Pradesh. Indian Pediatrics. 1987;24(10):903-06.
- [Google Scholar]
- Breastfeeding behavior of Indian women. Indian Journal of Community Medicine. 2004;29(2):62-64.
- [Google Scholar]
- The determinants of exclusive breast feeding in urban slums: a community based study. Journal of Tropical Pediatrics. 2009;55(1):49-54.
- [CrossRef] [PubMed] [Google Scholar]
- Gap between awareness and practices regarding maternal and child health among women in an urban slum community. Indian Journal of Pediatrics. 2008;75(5):455-58.
- [CrossRef] [PubMed] [Google Scholar]
- Breastfeeding practices in urban community of Surat city. National Journal of Community Medicine. 2010;1(2):111-13.
- [Google Scholar]
- India's progress towards the Millennium Development Goals 4 and 5 on infant and maternal mortality. WHO South-East Asia Journal of Public Health. 2012;1(3):279-89.
- [CrossRef] [PubMed] [Google Scholar]
- Juggling work and breastfeeding: effects of maternity leave and occupational characteristics. Pediatrics. 2009;123(1):38-46.
- [CrossRef] [PubMed] [Google Scholar]
- Does maternal employment affect breastfeeding? American Journal of Public Health. 1989;79(9):1247-50.
- [CrossRef] [PubMed] [Google Scholar]
- Infant feeding practices and associated factors through the first 9 months of life in Bavaria, Germany. Journal of Pediatric Gastroenterology and Nutrition. 2009;49(4):467-73.
- [CrossRef] [PubMed] [Google Scholar]
- Factors associated with weaning in the first 3 months postpartum. The Journal of Family Practice. 2002;51(5):439-44.
- [Google Scholar]
- Support for breastfeeding mothers. Cochrane Database of Systematic Reviews. 2007;1:CD001141.
- [CrossRef] [Google Scholar]
- Low-income mothers' views on breastfeeding. Social Science and Medicine. 2000;50(10):1457-73.
- [CrossRef] [PubMed] [Google Scholar]
- Exclusive breastfeeding- the relationship between maternal perception and practice. Nigerian Journal of Clinical Practice. 2009;12(4):403-06.
- [Google Scholar]
- Factors influencing the decision to breastfeed. Journal of Advanced Nursing. 2004;46(4):369-79.
- [CrossRef] [PubMed] [Google Scholar]
- Maternal employment, breastfeeding an. health: evidence from maternity leave mandates. Journal of Health Economics. 2008;27(4):871-87.
- [CrossRef] [PubMed] [Google Scholar]



