

Translate this page into:
Global Inequalities in Youth Mortality, 2007-2012
✉Corresponding author email: gsingh@mchandaids.org
Abstract
Objectives:
There is limited cross-national research on youth mortality. We examined age- and gender- variations in all-cause mortality among youth aged 15-34 years across 52 countries.
Methods:
Using the 2014 WHO mortality database, mortality rates for all countries were computed for the latest available year between 2007 and 2012. Rates, rate ratios, and ordinary least squares (OLS) and Poisson regression were used to analyze international variation in mortality.
Results:
Mortality rates among youth aged 15-34 years varied from a low of 28.4 deaths per 100,000 population for Hong Kong to a high of 250.6 for Russia and 619.1 for South Africa. For men aged 15-34, Singapore and Hong Kong had the lowest mortality rates (≈40 per 100,000), compared with South Africa and Russia with rates of 589.7 and 383.3, respectively. Global patterns in mortality among women were similar. Youth aged 15-24 in South Africa had 14 times higher mortality and those in the Philippines, Mexico, Russia, Colombia, and Brazil had 5-7 times higher mortality than those in Hong Kong. Youth aged 25-34 in Russia and South Africa had, respectively, 10 and 29 times higher mortality than their counterparts in Hong Kong. United States (US) had the 12th highest mortality rate among youth aged 15-24 and the 13th highest rate among youth aged 25-34. Overall, the US youth had 2-3 times higher rates of mortality than their counterparts in many industrialized countries including Hong Kong, Singapore, Netherlands, Switzerland, Germany, Norway, and Sweden. Income inequality, unemployment rate, and human development explained 50-66% of the global variance in youth mortality. Compared to the countries with low unemployment and income inequality and high human development levels, countries with high unemployment and income inequality and low human development had, respectively, 343%, 213%, and 205% higher risks of youth mortality.
Conclusions and Global Health Implications:
Marked international disparities in youth all-cause mortality largely reflect differences in violence and injury deaths and in such risk factors as unemployment, income inequality, human development, and alcohol consumption. The US ranks in the upper quartile of allcause mortality, with youth in Canada and many western industrialized countries showing significantly lower mortality risks than the US youth.
Keywords
Youth mortality
Human development
Global pattern
Unemployment
Inequality

Introduction
Youth aged 15-34 years are a major demographic group globally. They represent 27% of the total population in developed countries, 34% of the population in developing countries, and 33% of the total population globally.[1-3] Unintentional injuries (mostly motor vehicle accidents), homicide, and suicide are the three leading causes of youth mortality globally, with cardiovascular diseases, cancer, and infectious diseases including HIV/AIDS contributing additionally to premature mortality among the youth.[2-6] Indeed, risks of mortality from homicide, motor vehicle accidents, and firearm injuries among youth exceed those for the other age groups.[2-6]
Higher mortality risks among youth in most societies are generally linked to adverse social and economic conditions as youth are more likely than other groups to experience higher levels of poverty, unemployment, social disruption, migration, and risky behaviors (e.g., smoking, heavy drinking, and drug use), and lower levels of social participation and civic engagement.[2-5] Issues of increasing joblessness, limited employment opportunities, rising poverty, and social unrest among the youth, particularly in the context of the recent global economic crisis that started in 2008, pose a critical challenge for the health and social well-being of youth in many countries.[3,5,7,8] As such, analyses of the latest global patterns in youth mortality are urgently needed.
Even though youth represent a major segment ofthe global workforce, research examining cross-national disparities in youth mortality is limited. A recent study documented substantial variations in all-cause and cause-specific youth mortality rates across 45 industrialized countries for the 2003-2007 time period,[4] while another study looked at long-term trends in cause-specific youth mortality from 1955 to 1994 across 26 industrialized countries.[5] Two other studies examined trends and patterns in adolescent and young adulthood mortality according to world regions, including regions consisting of low- and middle-income countries.[6,9] Although youth suicide and homicide mortality patterns have been related to unemployment and socioeconomic factors,[2-4,10-13] the extent to which overall youth mortality rates in industrialized and developing countries vary in relation to human development, economic inequality, unemployment level, and health-risk behaviors such as hypertension, diabetes, obesity, and smoking have not yet been examined.
In this paper, using the latest international mortality statistics, we examine age- and gender- variations in all-cause mortality among youth aged 15-34 years across 52 developed and developing countries. We also analyze human development, socioeconomic, and behavioral determinants of international variation in youth mortality at the aggregate level.
Methods
Data for international comparisons of youth mortality came from the World Health Organization's (WHO) mortality database.[14] The WHO database provides global population and mortality data by age, sex, country, year, and cause of death, with information being provided by the civil registration systems of United Nations (UN) member states.[14] The 52 countries that were chosen were selected based on quality and completeness of data as well as the Organisation for Economic Co-operation and Development (OECD) member status and projected economic development.[4,14] Due to small number of deaths, mortality rates for Iceland were computed for 2007-2009 and for Luxembourg for 2009-2011 in order to produce stable rates. For all other countries, mortality rates were computed for a single calendar year between 2008 and 2012. Mortality data for the United States were for 2011.[15,16] Deaths, populations, and mortality rates for each country were derived for males, females, and all youth aged 15-24, 25-34, 15-34 years.
In addition to identifying countries that were at high risk of youth mortality, we modeled international variation in mortality as a function of human development index (HDI), gross national product (GNP) per capita, income inequality (Gini index), youth unemployment rate, alcohol consumption (measured as liters of pure alcohol per person per year for adults aged ≥15), and diabetes prevalence (raised blood glucose among adults).[3,4,10,17-20]
Other risk factors such as hypertension (raised blood pressure among adults aged ≥25) and obesity prevalence (among adults aged ≥20) were also considered, but, because of multi-collinearity, only their bivariate effects on youth mortality are shown.[17] Smoking was not related to youth mortality and was excluded from analyses. The data on the social and economic determinants and health- risk factors came from various UN data sources as well as the 2014 World Health Statistics Report and were nearest to the 2008-2012 time period.[8,17,18,20]
Human development index, developed by the United Nations Development Programme, is a composite index of social and economic development and combines indicators of life expectancy, educational attainment, and gross national income per capita. HDI varies between 0 and 1, with 0 indicating the lowest level and 1 representing the highest level of development.[18] We used both continuous and categorical definitions of key covariates. Three unemployment-rate categories were considered: <10% (i.e., referred to as the low-unemployment group), 10.0-31.9%, and >32% (referred to as the high-unemployment group). Gini coefficient was categorized into 3 groups: <0.32, 0.32-0.49, and ≥0.50. HDI was classified into three categories: <0.75, 0.75-0.87, and ≥0.88.
We used bivariate and multivariate ordinary least squares (OLS) regression models to estimate the impact of covariates on youth mortality rates. We used Poisson regression to model age-sex-country- specific deaths and population estimates as a function of socioeconomic, human development, and health-risk factors. The OLS models were estimated by the SAS REG procedure,[21] while Poisson models were estimated by the SAS GENMOD procedure.[22] Differences in mortality rates, rate ratios, and relative risks were tested for statistical significance at the 0.05 level.
Results
International Disparities in Mortality among Youth Aged 15-34
Mortality rates among youth aged 15-34 years varied from a low of 28.4 deaths per 100,000 population for Hong Kong to a high of 250.6 for Russia and 619.1 for South Africa (Figure 1). For men aged 15-34, Singapore and Hong Kong had the lowest mortality rates (≈40 per 100,000), compared with South Africa and Russia with rates of 589.7 and 383.3, respectively (Figure 2). Global patterns in mortality among women aged 15-34 were similar, with South Africa and Russia having the highest rates and Hong Kong and Israel the lowest rates. Overall, the US youth had 2-3 times higher rates of mortality than their counterparts in many industrialized countries including Hong Kong, Singapore, Netherlands, Switzerland, Germany, Norway, and Sweden. The US youth had 62%, 76%, and 78% higher mortality than their counterparts in Canada, Australia, and the United Kingdom, respectively.
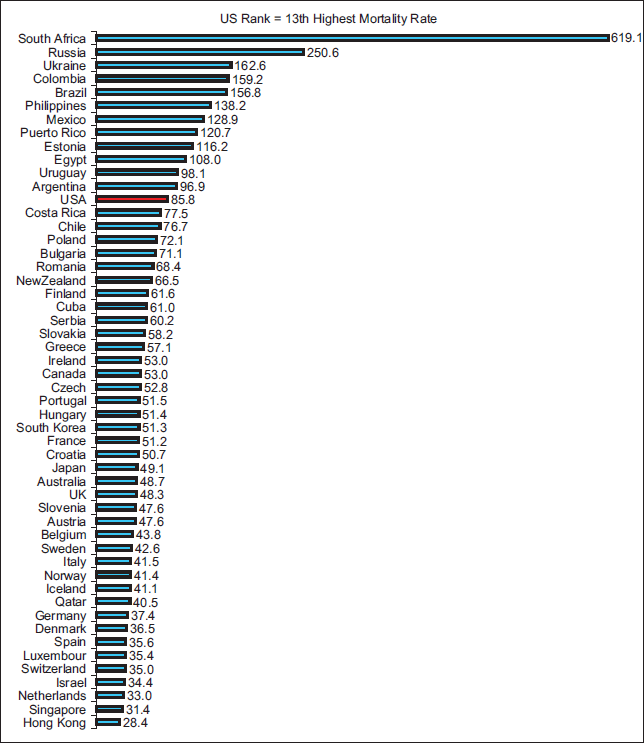
- All-Cause Mortality Rates per 100,000 Population, Youth Aged 15-34 Years, Selected Developed and Developing Countries, 2007-2012. Data for Iceland are pooled for the period 2007-2009 and for Luxembourg for the period 2009-2011. Data for all other countries are for a single calendar year between between 2008 and 2012.
-
Source: WHO Mortality Database, 2014 (http://www.who.int/ healthinfo/mortality_data/en/
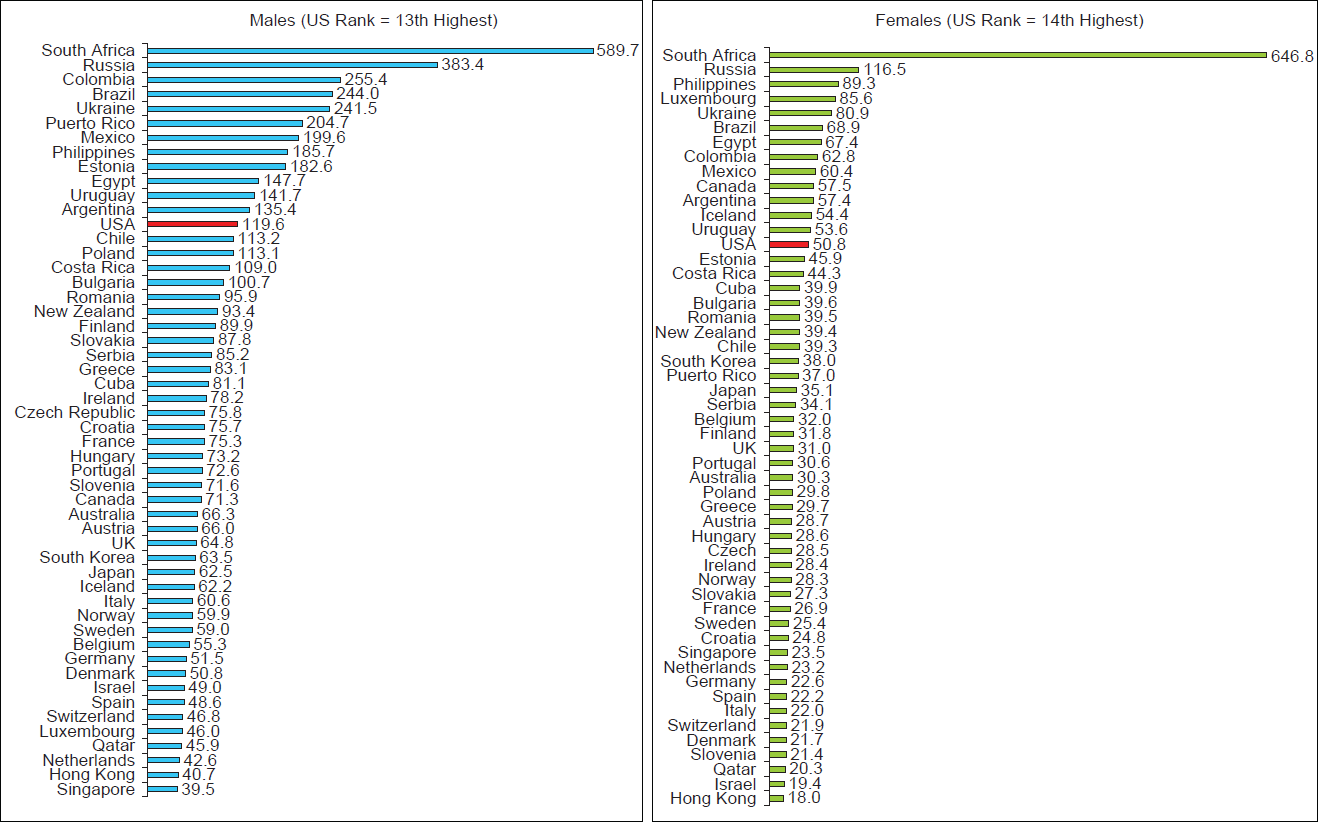
- All-Cause Mortality Rates per 100,000 Population, Male and Female Youth Aged 15-34 Years, Selected Developed and Developing Countries, 2007-2012. Data for Iceland are pooled for the period 2007-2009 and for Luxembourg for the period 2009-2011. Data for all other countries are for a single calendar year between between 2008 and 2012.
-
Source: WHO Mortality Database, 2014 (http://www.who.int/healthinfo/mortality_data/en/)
International Patterns in Mortality among Youth Aged 15-24 and 25-34 Years
Youth aged 15-24 in South Africa (with a rate of 293 deaths per 100,000 population) had 14 times higher mortality and those in the Philippines, Mexico, Russia, Colombia, and Brazil 5-7 times higher mortality than those in Hong Kong (rate = 20.6). Youth aged 25-34 in Russia (rate = 357.3) and South Africa (rate = 104.7) had, respectively, 10 and 29 times higher mortality than their counterparts in Hong Kong (rate = 34.7). Among the 52 countries examined, United States had the 12th highest mortality rate (67.7) among youth aged 15-24 and the 13th highest rate (104.7) among youth aged 25-34 (Figure 3).
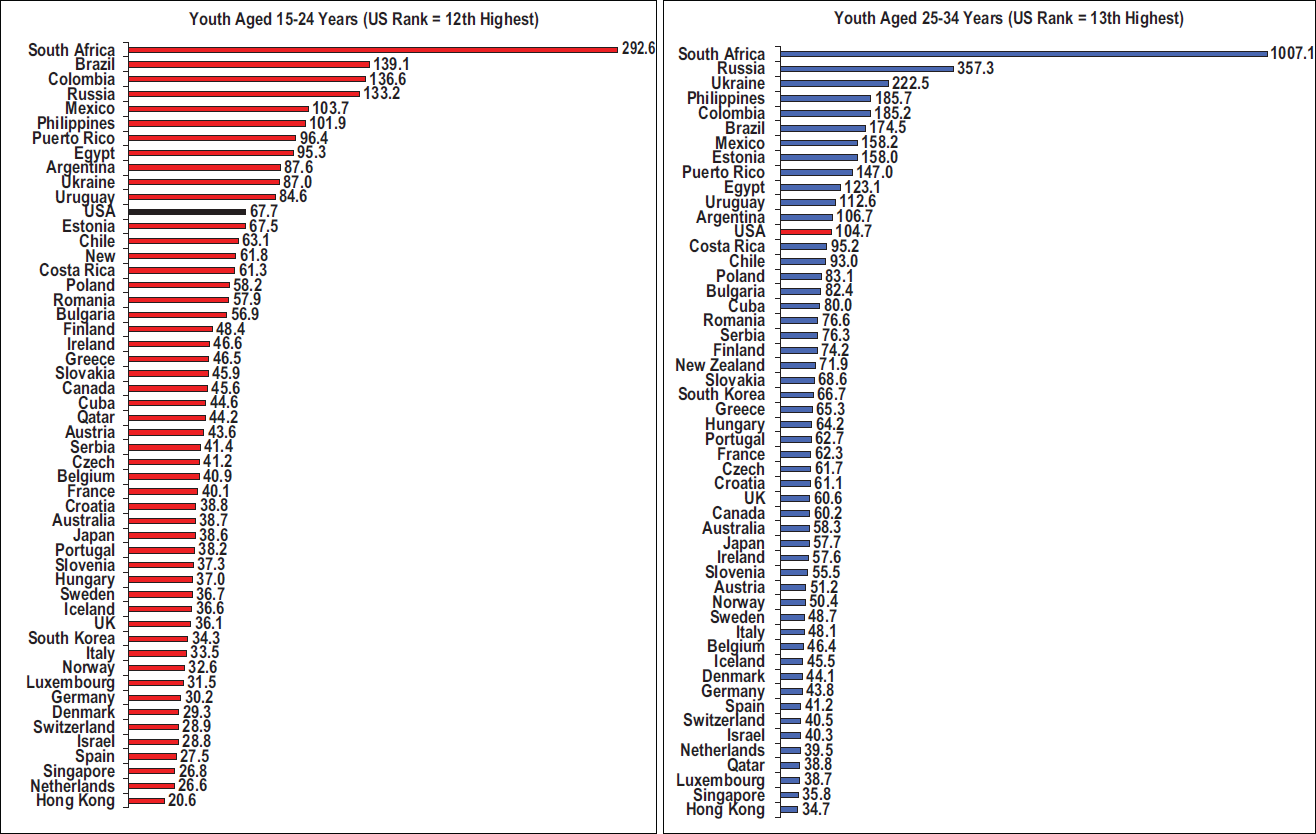
- All-Cause Mortality Rates per 100,000 Population, Youth Aged 15-24 and 25-34 Years, Selected Developed and Developing Countries, 2007-2012. Data for Iceland are pooled for the period 2007-2009 and for Luxembourg for the period 2009-2011. Data for all other countries are for a single calendar year between between 2008 and 2012
-
Source: WHO Mortality Database, 2014 (http://www.who.int/healthinfo/mortality_data/en/)
Modeling the Impact of Human Development and Socioeconomic Inequality on Global Youth Mortality
Gross national product per capita, HDI, income inequality, and unemployment rate were all significant predictors of youth mortality, with the latter three explaining 54.8% of the global variance in youth mortality aged 15-34 (Table 1). In the OLS models for youth aged 15-24 and 25-34 and for male and female youth aged 15-34, HDI, income inequality, and unemployment accounted for 66%, 50%, 60%, and 40% of the variance in mortality rates, respectively (data not shown). In the multivariate OLS model, HDI had the greatest relative impact on youth mortality. A 0.1 unit increase in HDI was on average associated with a 46-point decrease in the overall youth mortality rate and 62 and 28 points decrease in male and female youth mortality rates, respectively. A 5-percentage point increase in youth unemployment was associated with a 10-point increase in overall youth mortality, while a 0.1-unit increase in income inequality (Gini coefficient) was associated with a 31-point increase in youth mortality (Table 1). Diabetes, hypertension, and obesity prevalence were also significantly associated with increased youth mortality rates in bivariate models (Table 1). Alcohol consumption was significantly associated with youth mortality rates after controlling for HDI, income inequality, unemployment, and diabetes prevalence (data not shown).
| Covariate | b | β | t-statistic | P-value | R2 |
|---|---|---|---|---|---|
| Bivariate models | |||||
| Human Development Index (HDI)a | −71.47 | −0.65 | −6.01 | <0.001 | 42.47 |
| Gross National Product per capita (Intl $)b | −9.62 | −0.40 | −3.07 | <0.001 | 15.85 |
| Youth unemployment ratec | 18.35 | 0.42 | 3.31 | 0.002 | 17.93 |
| Income inequality (Gini index)d | 49.69 | 0.53 | 4.46 | <0.001 | 28.50 |
| Alcohol consumption per capitae | 8.91 | 0.07 | 0.51 | 0.613 | 0.01 |
| Diabetes prevalencef | 74.77 | 0.35 | 2.65 | 0.011 | 12.32 |
| Hypertension prevalenceg | 23.37 | 0.36 | 2.76 | 0.008 | 13.23 |
| Obesity prevalenceh | 16.38 | 0.27 | 1.96 | 0.050 | 7.16 |
| Multivariate models | |||||
| Model 1: Human Development Index + | −46.12 | −0.42 | −3.58 | <0.001 | 54.76 |
| Youth unemployment rate + | 10.39 | 0.24 | 2.25 | 0.029 | |
| Income inequality (Gini index) | 31.18 | 0.32 | 2.94 | 0.005 | |
| Model 2: GNP per capita + | −3.78 | −0.16 | −1.25 | 0.217 | 43.07 |
| Youth unemployment rate + | 12.67 | 0.29 | 2.39 | 0.021 | |
| Income inequality (Gini index) | 42.67 | 0.46 | 4.09 | <0.001 | |
Notes: b=Unstandardized regression coefficient, β=Standardized regression coefficient, R2=Percentage variance explained. β is also equal to the correlation coefficient in bivariate regression models. aIncrease in mortality rates associated with a 0.1 unit increase in HDI. bIncrease in mortality rates associated with a $5,000 increase in GNP per capita. cIncrease in mortality rates associated with a 5-percentage point increase in youth unemployment rate. dIncrease in mortality rates associated with a 0.1 unit increase in income inequality. eIncrease in mortality rates associated with a 5-percentage point increase in alcohol consumption. fIncrease in mortality rates associated with a 5-percentage point increase in raised blood sugar rates. gIncrease in mortality rates associated with a 5-percentage point increase in hypertension prevalence. hIncrease in mortality rates associated with a 5-percentage point increase in obesity prevalence
According to bivariate Poisson models, compared to countries with low unemployment and income inequality and high human development levels, countries with high unemployment and income inequality and low human development had, respectively, 343%, 213%, and 205% higher risks of youth mortality (Table 2). Alcohol consumption and diabetes, hypertension, and obesity prevalence were all significantly related to increased risk of youth mortality in bivariate models (Table 2). In the multivariate Poisson model, a 0.1 unit increase in human development was associated with 43% lower risk of youth mortality. Adjusting for human development, diabetes prevalence, and alcohol consumption, countries with high income inequality and unemployment levels had 42% and 56% higher risks of youth mortality respectively than countries with low income inequality and unemployment levels. Alcohol consumption per capita and diabetes prevalence were independently related to youth mortality, with each additional 5-percentage point increase in the two variables resulting in a 33% and 51% increase in youth mortality risk respectively (Table 2).
| Covariate | Relative risk RR | 95% confidence interval | P-value |
|---|---|---|---|
| Bivariate models | |||
| Human Development Index (HDI), continuousa | 0.57 | 0.56-0.57 | <0.001 |
| Human Development Index (HDI), categorical | |||
| <0.75 (low) | 3.05 | 3.03-3.07 | <0.001 |
| 0.75-0.87 | 1.09 | 1.08-1.09 | <0.001 |
| ≥0.88 (high) | Reference | ||
| Gross National Product per capita (Intl $)b | 0.89 | 0.89-0.89 | <0.001 |
| Youth unemployment rate, continuousc | 1.21 | 1.21-1.21 | <0.001 |
| Youth unemployment rate, categorical | |||
| <10.0% (low) | Reference | ||
| 10.0-31.9% | 1.57 | 1.55-1.58 | <0.001 |
| ≥32.0% (high) | 4.43 | 4.39-4.47 | <0.001 |
| Income inequality (Gini index), continuousd | 1.69 | 1.68-1.69 | <0.001 |
| Income inequality (Gini index), categorical | |||
| <0.32 (low) | Reference | ||
| 0.32-0.49 | 1.46 | 1.45-1.47 | <0.001 |
| ≥0.50 (high) | 3.13 | 3.11-3.16 | <0.001 |
| Alcohol consumption per capitae | 1.26 | 1.25-1.26 | <0.001 |
| Diabetes prevalencef | 2.01 | 2.00-2.02 | <0.001 |
| Hypertension prevalenceg | 1.55 | 1.55-1.55 | <0.001 |
| Obesity prevalenceh | 1.13 | 1.13-1.13 | <0.001 |
| Multivariate model | |||
| Human Development Index | 0.58 | 0.58-0.58 | <0.001 |
| Youth unemployment rate, categorical | |||
| <10.0% (low) | Reference | ||
| 10.0-31.9% | 1.16 | 1.15-1.17 | <0.001 |
| ≥32.0% (high) | 1.56 | 1.54-1.58 | <0.001 |
| Income inequality (Gini index), categorical | |||
| <0.32 (low) | Reference | ||
| 0.32-0.49 | 1.35 | 1.34-1.36 | <0.001 |
| ≥0.50 (high) | 1.42 | 1.40-1.43 | <0.001 |
| Alcohol consumption per capita | 1.33 | 1.32-1.33 | <0.001 |
| Diabetes prevalence | 1.51 | 1.50-1.52 | <0.001 |
aIncrease in mortality risk associated with a 0.1 unit increase in HDI. bIncrease in mortality risk associated with a $5,000 increase in GNP per capita. cIncrease in mortality risk associated with a 5-percentage point increase in youth unemployment rate. dIncrease in mortality risk associated with a 0.1 unit increase in income inequality. eIncrease in mortality risk associated with a 5-percentage point increase in alcohol consumption. Increase in mortality risk associated with a 5-percentage point increase in raised blood sugar rates. gIncrease in mortality risk associated with a 5-percentage point increase in hypertension prevalence. hIncrease in mortality risk associated with a 5-percentage point increase in obesity prevalence
Discussion
Although international variations in youth mortality have been examined previously,[4,5,6,9] our study extends previous analyses by providing a comprehensive analysis of factors underlying crossnational disparities in youth mortality across a large number of industrialized countries and selected developing countries. Our analysis shows substantial global disparities in mortality, with youth in South Africa, Russia, Ukraine, Colombia, and Brazil having the highest risk of premature mortality and those in Hong Kong, Singapore, and Netherlands having the lowest risk. United States ranks in the upper quartile of youth mortality, having markedly higher mortality rates than all other high-income countries, including Netherlands, Germany, France, UK, Japan, and Australia.
Our study highlights the critical role of human development, inequality, and unemployment in explaining cross-national variations in overall youth mortality. While the estimation of the health impact of human development among youth is new, the estimated effects of socioeconomic inequality and unemployment on youth mortality reported in our study are compatible with those from previous studies on youth mortality, including mortality rates from homicide, suicide, and unintentional injuries.[2-4,10-13] Two possible mechanisms underlying these associations can be proposed. Firstly, youth unemployment and income inequality increase the risk of social unrest at the societal level, which, in turn, could lead to increased violence and mortality among the youth.[8] Secondly, lack of social integration leads to increased youth suicide and homicide rates, and societies or communities with lower levels of social integration and cohesiveness, as measured by higher socioeconomic inequality and unemployment levels, have higher rates of violence and mortality, a pattern compatible with Durkheim's theory of social integration.[23,24]
International disparities in youth mortality reflect differences in deaths due to violence and unintentional injuries as well as deaths from cardiovascular disease, cancer, and HIV/AIDS.[4,5,14] Cross-national analyses of cause-specific youth mortality patterns can identify more precisely the effects of human development, socioeconomic factors, and behavioral determinants. For the 52 countries combined, unintentional injuries (mostly motor vehicle accidents), homicides, and suicides accounted for approximately 40% of all deaths among youth.[14] Nearly 11% of the youth deaths were due to cancer and cardiovascular disease,[14] which indicates the significant role of lifestyle factors such as obesity, physical inactivity, hypertension, and raised blood-sugar levels in contributing to the global disease burden among youth. Relative contribution of these causes to overall youth mortality in a specific country can vary greatly depending upon the level of industrialization, urbanization, and national wealth. While for many western industrialized and high- income countries, these causes account for 70-80% of all youth deaths, for middle-income countries such as South Africa and Egypt, they account for 9% and 29% of deaths respectively.[14] Infectious and parasitic diseases including malaria, tuberculosis, hepatitis, and HIV/AIDS account for over 37% of all youth deaths in South Africa.[14] Moreover, for a number of Latin American countries, violence accounts for a substantial proportion of all youth deaths; about half of all youth deaths in Puerto Rico and Colombia are due to homicide.[14] Indeed, youth violence is a major public health problem worldwide, and contributes greatly to the global burden of premature mortality, injury, and disability.[19,25] Youth suicides are a major concern in many high-income countries, as 33-43% of all youth deaths in South Korea, Japan, Hong Kong, and Finland are attributed to suicide.[14]
Unintentional injuries, especially transport- related, are the leading cause of death among youth globally.[4,5,6,26] More than half of all traffic deaths occur among youth aged 15-34.[14,26] Middle-income countries are most affected by traffic deaths among youth, and the African region has the highest road traffic fatality rate.[26] Trends in motor-vehicle injury deaths indicate declining mortality rates for most high-income countries, while, for many low- and middle-income countries, motor-vehicle or traffic- related injury deaths are on the rise.[26] Differences in youth mortality from transport-related injuries reflect large cross-national disparities in the legislation, enforcement, and use of seat belts, reduced drink-driving, speed limits, motor-vehicle safety improvements, and road conditions.[26] Noncommunicable diseases such as cardiovascular disease and cancer are a growing threat to the health of young people globally, and the rising epidemic of obesity and smoking, if not curbed, can substantially influence future trends in youth mortality, particularly in low- and middle-income countries.[17,27]
The WHO mortality database, on which our study is based, provides mortality statistics for a limited number of countries with fairly complete and accurate civil registration systems.[14] Reliable all-cause youth mortality data are, however, available for many additional developing countries from the UN annual demographic yearbook, which compiles data from various national civil registration systems, censuses, or household surveys.[28] For example, the 2011 estimated mortality rates for youth aged 15-34 in China and India were 57 and 175, respectively. Recent youth mortality rates for Malawi, Zambia, Sierra Leone, and Swaziland were 663, 847, 1023, and 1,920 respectively, which are almost as high as or higher than the rate reported for South Africa. Future studies may benefit from including youth mortality data for these additional low- and middle-income countries and by examining the impact of human development, social inequality, and unemployment on youth mortality for a wider set of countries than those shown in our study.
Conclusions and Global Health Implications
Human development, income inequality, and unemployment are powerful determinants of youth mortality at the global level. High levels of social and economic inequality contribute greatly to increased premature mortality among youth both within and across countries, with significant adverse consequences for global population health and development.[2-5,10,17,27] To reduce youth mortality, public policies must emphasize greater investments in human development and provide greater social protection, welfare support, and increased educational and labor market opportunities for the vulnerable youth in both developed and developing countries.[4,7,8,17,18] The recent global economic crisis has led to increases in youth unemployment levels in both developed and developing countries, but, since 87% of the world's youth live in developing countries who lack social safety nets and social protection measures enjoyed by their counterparts in the developed world, the health impacts of rising unemployment and diminishing labor market opportunities have likely been greater among youth in developing economies.[7,8]
Human Subjects Review:
No IRB approval was required for this study, which is based on the secondary analysis of public-use United Nations databases.
Financial Disclosure:
None to report.
Acknowledgments:
The views expressed are the authors’ and not necessarily those of the Global Health and Education Projects or any of the authors affiliated institutions.
Conflicts of Interest:
None.
Funding/Support:
None.
References
- Bureau. International Database 2010 http://www.census.gov/population/international/data/idb/informationGateway.php
- [Google Scholar]
- Trends and differentials in adolescent and young adult mortality in the United States, 1950 through 1993. American Journal of Public Health. 1996;86(4):560-564.
- [CrossRef] [PubMed] [Google Scholar]
- Youth Mortality in the United States, 1935-2007: Large and Persistent Disparities in Injury and Violent Deaths. A 75th Anniversary Publication. Health Resources and Services Administration, Maternal and Child Health Bureau 2010 http://www.mchb. hrsa.gov/
- [Google Scholar]
- All-cause and cause-specific mortality among US youth: socioeconomic and rural-urban disparities and international patterns. Journal of Urban Health. 2013;90(3):388-405.
- [CrossRef] [PubMed] [Google Scholar]
- An international comparison of adolescent and young adult mortality. Annals of the American Academy of Political and Social Science. 2002;580:172-200.
- [CrossRef] [PubMed] [Google Scholar]
- Global patterns of mortality in young people: a systematic analysis of population health data. Lancet. 2009;374(9693):881-892.
- [CrossRef] [PubMed] [Google Scholar]
- United Nations. New York, USA: World Youth Report; 2013. http://unworldyouthreport.org/
- [Google Scholar]
- World of Work Report 2013: Repairing the Economic and Social Fabric. Geneva, Switzerland: International Labour Office; 2013.
- [CrossRef] [Google Scholar]
- 50-year mortality trends in children and young people: a study of 50 low-income, middle-income, and high-income countries. Lancet. 2011;377(9772):1162-1174.
- [CrossRef] [PubMed] [Google Scholar]
- Sex- and age-specific relations between economic development, economic inequalit. and homicide rates in people aged 0-24 years: a cross-sectional analysis. Bulletin of the World Health Organization. 2002;80(10):797-805.
- [Google Scholar]
- Suicide rates in young men in England and Wales in the 21st century: time trend study. British Medical Journal. 2008;336(7643):539-542.
- [CrossRef] [PubMed] [Google Scholar]
- Suicide and unemployment in young people: analysis of trends in England Wales, 1921-1995. British Journal of Psychiatry. 1999;175:263-270.
- [CrossRef] [PubMed] [Google Scholar]
- Crime and unemployment among youth in the United States, 1958-1990: A time series analysis. American Journal of Economics and Sociology. 1994;53(1):99-109.
- [CrossRef] [Google Scholar]
- WHO Mortality Database. 2014 Available at: http://www.who.int/healthinfo/mortality_data/en/ (accessed )
- [Google Scholar]
- National Vital Statistics System, Mortality Multiple Cause-of-Death Public Use Data File Documentation. Hyattsville, MD: US Department of Health and Human Services 2014 Available at: http://www.cdc.gov/nchs/nvss/mortality_ public_use_data.htm (accessed )
- [Google Scholar]
- SAS/STAT Users Guide, Version 9.1: The REG Procedure. Cary, NC: SAS Institute Inc.; 2004.
- [Google Scholar]
- SAS/STAT Users Guide, Version 9.1: The GENMOD Procedure. Cary, NC: SAS Institute Inc.; 2004.
- [Google Scholar]
- Social integration and mortality in Australia. Australian and New Zealand Journal of Public Health. 1999;23:571-577.
- [CrossRef] [PubMed] [Google Scholar]
- Health and Social Factors in Kansas. In: Singh GK, Wilkinson AV, Song FF, Rose TP, Adrian M, Fonner E, Tarlov A, eds. Kansas Health Institute. Lawrence, KS: Allen Press; 1998.
- [Google Scholar]
- World Report on Violence and Health. Geneva, Switzerland: World Health Organization 2002
- [CrossRef] [PubMed] [Google Scholar]
- Global Status Report on Road Safety 2013: Supporting a Decade of Action. Geneva, Switzerland 2013
- [Google Scholar]
- The Growing Danger of Non-Communicable Diseases: Acting Now to Reverse Course. 2011.
- [Google Scholar]



