

A Surveillance System for the Maternal and Child Health (MCH) Population During the COVID-19 Pandemic
* Corresponding author email: veronicaajewole@yahoo.com
-
Received: ,
Accepted: ,
This is an open-access article distributed under the terms of the Creative Commons Attribution-Noncommercial-Share Alike 3.0 Unported, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Abstract
Severe Acute Respiratory Syndrome Coronavirus 2 (SARS-CoV-2), the causative agent for coronavirus disease 2019 (COVID-19), and its ensuing mitigation measures have negatively affected the Maternal and Child Health (MCH) population. There is currently no surveillance system established to enhance our understanding of SARS-CoV-2 transmission to guide policy decision making to protect the MCH population in this pandemic. Based on reports of community and household spread of this novel infection, we present an approach to a robust family-centered surveillance system for the MCH population. The surveillance system encapsulates data at the individual and community levels to inform stakeholders, policy makers, health officials and the general public about SARS-CoV-2 transmission dynamics within the MCH population.
Keywords
COVID-19
Coronavirus
Maternal and child health
Family-centered
Surveillance system
Individual level data elements
Community level data elements
Community transmission of SARS-CoV-2

1. Introduction
Severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) is a novel coronavirus that causes coronavirus disease 2019 (COVID-19), a respiratory disease that exhibits a wide range of clinical outcomes from asymptomatic and mild disease to severe viral pneumonia, Acute Respiratory Distress Syndrome (ARDS), Multisystem Inflammatory Syndrome in Children (MIS-C), acute kidney injury, thrombotic disorders and serious cardiac, cerebrovascular and vascular complications.1 Since the first reported cases in China in December 2019, more than 12 million cases of COVID-19 have been reported globally, including more than 566,000 deaths from over 200 countries thus, leading to a global pandemic.2 To mitigate the spread of SARS-CoV-2, stringent measures such as lock-downs, limited access to healthcare resources, school closures, stay-at-home orders, among others, were implemented across the United States and globally.3 Although there is sparse evidence about SARS-CoV-2 infection risk among that the Maternal and Child Health (MCH) population, these COVID-19 mitigation measures have significantly impacted this population including reduced access to prenatal/postpartum care, transportation, medical abortion care, newborn care, children vaccination as well as socio-economic distress from job-loss and home-schooling. 4 Previous research indicates that surveillance systems help health officials to understand disease distribution and respond to them effectively.5 It is, therefore, imperative to establish a surveillance system to track and monitor COVID-19 disease progression and its impact within the MCH population.
Similar to the Pregnancy Risk Assessment Monitoring System, Zika Postpartum Emergency Response Survey (PRAMS-ZPER)6 system, and the Influenza Hospitalization Surveillance Network (FluSurv-NET),7 a robust family-centered surveillance system for the MCH population during the COVID-19 pandemic will help to determine risk profiles, define predictors of disease severity grades and guide recommendations for treatment and vaccination programs for COVID-19 within the MCH population.
2. Methodological Approach
COVID-19 clinical reports have defined person-to- person transmissions within the MCH population in which infected individuals could spread the disease even before onset of symptoms.3 Repeated contact and close spatial proximity with infected individuals in the household environment makes the household the epicenter for SARS-CoV-2 transmission. 8 Given this premise, capturing data elements that will reflect the dynamics of SARS-CoV-2 transmission at the individual and community level becomes important. Additionally, inclusion of data elements from symptomatic and asymptomatic family individuals could assist in understanding predictors of transmission as well as patterns of resilience and vulnerability.
To simplify the approach in the development of this robust family-centered surveillance system, type 1 and 2 database infrastructures will be adopted. Type 1 database infrastructure will consist of individual level data elements while type 2 database infrastructure will comprise of individual and community level data elements. Individual level data elements will encompass socio-demographic characteristics, health information, and travel information while community level data elements include information about the built environment, resource availability, and social behaviors. Information at the individual level will give insight into the natural history of COVID-19 disease, progression, complications during pregnancy, and the post-partum period as well as among family adults, infants and children. The community level information will improve our understanding regarding drivers of community transmission and environmental factors influencing disease occurrence, spread and outcomes including resultant COVID-19 racial/ethnic disparities. Data elements collected from either the type 1 or type 2 database infrastructure will be reported to local, state, and federal government and non-governmental agencies for MCH public health policy making and assurance. The data in this robust family-centered surveillance system will be made publicly-available to all stakeholders including academic and non-academic researchers, governmental, non-governmental and private agencies as well as other individual entities.
3. Results
The framework of the COVID-19 family-centered surveillance system is shown in Figure 1. Health information at the individual level consisted of socio-demographic characteristics, health information, and travel information. Socio-demographic characteristics included age, education, race/ethnicity, gender, household income, language literacy, essential or remote worker status, social support, interactional practices (the degree of exchange between household members), and housing status. Housing structure data revealed if a person lived in an apartment, house or was experiencing homelessness. Health characteristics comprised of test results, immunity status, comorbidities, time of active infection, severity of disease, medical intervention, treatment received, availability of personal protective equipment, and insurance status. Travel information contained data on travel history and immigration status.
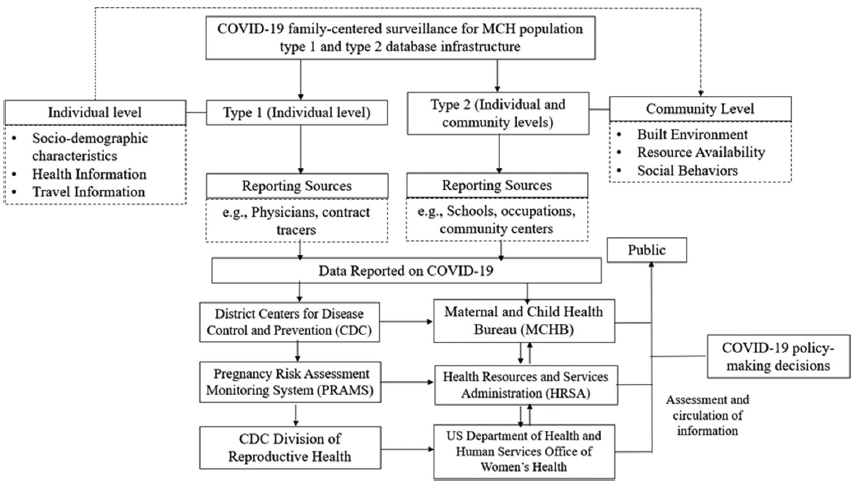
- Type 1 and Type 2 framework of a family-centered COVID-19 surveillance system for the MCH population
Community-level health data included information about the built environment, resource availability, and social behaviors. The built environment included region, location, spatial proximity index, residential segregation, neighborhood deprivation, and air pollution index. Resource availability data encompassed neighborhood zip code income, availability of testing centers, community partners and other community resources. Social behaviors comprised of close-proximity activism and the degree of social distancing.
4. Discussion, Conclusion and Global Health Implications
The surveillance system for the MCH population during the COVID-19 pandemic proposed in this study could be utilized to inform stakeholders, policy makers, and health officials. This study provides a template on how to effectively serve vulnerable populations within our society during COVID-19 by creating a two- tiered family-centered surveillance system. Routine data evaluations of this robust surveillance system would be conducted to increase its efficiency and effectiveness, modify the roles of relevant stakeholders, the analysis and interpretation of surveillance data, approaches to system monitoring and evaluation, and opportunities for future advances in terms of increased scientific rigor, outcomes-focused research, and health informatics.
Acknowledgements:
Not applicable.
Compliance with Ethical Standards
Conflicts of Interest: None from all authors and co-authors.
Financial Disclosure: None from all authors and co-authors.
Funding/Support: This work was funded by the Health Resources and Services Administration’s Maternal and Child Health Student Training Program (HRSA-MCH; T16MC29831).
Ethics Approval: Not applicable.
References
- Coronavirus disease 2019 (COVID-19) treatment guidelines. https://www.covid19treatmentguidelines.nih.gov
- COVID-19 Case Tracker. https://coronavirus.jhu.edu
- Coronavirus (COVID-19). https://www.cdc.gov/coronavirus/2019-ncov/index.html
- Amidst the COVID-19 pandemic, we must remember maternal health. https://www.mhtf.org/2020/04/18/amidst-the-covid-19-pandemic-we-must-remember-maternal-health/
- Public health surveillance systems:recent advances in their use and evaluation. Annual Review of Public Health. 2017;38:57-79.
- [Google Scholar]
- PRAMS Zika postpartum emergency response survey (PRAMS-ZPER) in Puerto Rico. https://www.cdc.gov/prams/special-projects/zika/index.htm
- The US influenza Hospitalization Surveillance Network. Emerging Infectious Diseases –Center for Disease Control and Prevention. 2015;21(9):1543-1550. doi:10.3201/eid2109.141912
- [Google Scholar]
- Characteristics of household transmission of COVID-19. Clinical Infectious Diseases 2020:ciaa450. https://doi.org/10.1093/cid/ciaa450
- [Google Scholar]



