

Translate this page into:
Vaccination Coverage Under the Expanded Program on Immunization in South West Cameroon
*Corresponding author email: ngwayuclaude1@gmail.com
-
Received: ,
Accepted: ,
This is an open-access article distributed under the terms of the Creative Commons Attribution-Noncommercial-Share Alike 3.0 Unported, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Abstract
Background:
Inadequate vaccination coverage with increased risk of vaccine preventable disease outbreaks remain a problem in Africa. The aim of this study was to assess the vaccination coverage levels under the Expanded Program on Immunization (EPI) in a health area and to identify factors that affect vaccination coverage in view of providing valuable data for disease prevention.
Methods:
A cross-sectional household survey was conducted in August 2017 in the Mbonge health area, Southwest Cameroon. Clustered sampling technique was used to select study communities and a purposive sampling design was used to select households. An interviewer-administered questionnaire was used to obtain information from consenting caregivers of children aged 9–23 months. Vaccination coverage was assessed by consulting the vaccination cards and parents’ recall. In households with more than one child aged 9-23months, the youngest was chosen.
Results:
Overall, 300 caregivers were enrolled into the study. The average vaccination coverage for the past three years (2014-2016) was 34.0%. Two hundred and fifty-five (85%) children had vaccination cards. Amongst the children, 143 (47.7%) had taken all vaccines as recommended while 30 (10%) had not received a single dose. Factors significantly associated with incomplete vaccination status included: occupation (being a farmer) (p-value=0.011), marital status (married) (p-value=0.048), caregiver’s utilization of health facility (p-value=0.003), low levels of mothers’ utilization of antenatal care (ANC) services (p-value=0.000), and low knowledge on vaccination (p-value=0.000).
Conclusion and Global Health Implications:
Adequate vaccination coverage can be attained through good sensitization and health education for primary caregivers. Targeting families living far away from vaccination centers, using appropriate communication and vaccination strategies may improve vaccination coverage in the Mbonge Health Area of South West Region, Cameroon.
Keywords
Assessment
Vaccination Coverage Expanded Program on Immunization
Mbonge Health Area
Cameroon
EPI

1. Introduction
Vaccination is one of the most effective, inexpensive, and cost-effective intervention strategies to reduce maternal and child morbidity and mortality from several infectious diseases.1 Globally, over two million deaths are delayed through vaccination each year.2 However, vaccine preventable diseases (poliomyelitis, measles, tetanus and yellow fever) remain the most common cause of childhood mortality with an estimated three million deaths each year.3 The World Health Organization (WHO) initiated the expanded program on immunization (EPI) in May 1974 with the objective to vaccinate children throughout the world.4 Six vaccine-preventable diseases were initially included in the EPI namely: tuberculosis, poliomyelitis, diphtheria, tetanus, pertussis and measles. As time went by, increased knowledge of the immunologic factors of diseases led to the development and addition of new vaccines to the EPI’s list of recommended vaccines such as hepatitis B and yellow fever in countries endemic for the disease and Haemophilus influenzae meningitis (Hib) conjugate vaccine in countries with high burden of disease.3 In 2018, Global efforts had immunized about 86% of infants worldwide with three doses of diphtheria-tetanus-pertussis (DPT) about 86% of infants worldwide (116.3 million infants) received 3 doses of diphtheria-tetanus-pertussis (DTP3) vaccine, 89% had received BCG and 86% had received the first dose of the measles vaccine.5 Despite the safe, effective and inexpensive nature of vaccines, national childhood immunization program coverage for vaccine preventable diseases remain insufficient in many African countries and the reoccurrence of epidemics still occur.
In October 2013, there was an outbreak of polio in the Western region (Dschang Health District) of Cameroon where wild polio type 1 was isolated from two acute flaccid paralysis cases.6 Four cases due to circulating vaccine-derived poliovirus type 2 were reported in the far northern region of Cameroon specifically in the city of Mada. According to the Global Polio Eradication Initiative, a total of 9 cases of wild polio virus-1 have been reported in Cameroon in the years 2013-2014 and this represent the first polio outbreak reported in the country since 2009 (Global Polio Eradication Initiative, 2015).
In 2008, the measles surveillance system in Cameroon, consisting of weekly morbidity and mortality reports compiled by the Ministry of Health, identified an increased number of measles cases in the Northern city of Maroua. Despite reinforcement of routine vaccination activities in 2008 and two vaccination interventions conducted in October 2008 and January 2009 in response to the epidemic, cases continued to be reported.7 Another measles outbreak occurred between March and May 2015 in Misaje, a health area under Nkambe health district, where a total of 6 cases were diagnosed and investigated.8 In March 2016, there was rumor of a measles outbreak in the Mbonge health area; a team was consequently sent from the Buea Regional Delegation of Public Health (BRDPH) to investigate the outbreak. Five suspected cases were detected, samples were collected and sent to Centre Pasteur in Yaounde where they were confirmed to be measles. In order to assess the vaccination coverage levels of vaccines on the expanded program on immunization (EPI) in the Mbonge health area for the past three years (2014 to 2016) and associate it to the possible cause of the measles outbreak in the area, questionnaires were administered to caregivers to identify factors that affect vaccination coverage in this area. Vaccination coverage levels for the past three years (2014 and 2016) were assessed by review of hospital records to calculate percentage coverage and administered questionnaires to caregivers to identify factors that affect vaccination coverage in the Mbonge Health Area, South West Cameroon.
1.1. Objectives of the Study
The objective of this study was to assess the vaccination coverage levels of vaccines under the EPI in Mbonge health area and identify factors that affect vaccination coverage in view of providing valuable data for disease prevention. The specific objectives of the study were to: determine the EPI vaccination coverage levels in Mbonge Health area; identify the factors that affected the EPI vaccination coverage levels in Mbonge health area; and investigate the possible existence of an association between vaccination coverage and incidence of measles under the EPI.
Information on vaccination coverage from this study will indicate whether substantial efforts were being made to achieve vaccination targets in Mbonge Health District. Also, the information on factors affecting vaccination coverage will give indication to potential causes of the measles outbreak in that health area, and this would determine whether vaccination strategies or interventions need to be revised or changed completely.
2. Methods
2.1. Study Design, Population and Setting
The study was a cross sectional community-based survey involving members of households selected by clustered and purposive sampling technique. Records on vaccination from 2014- 2016 from the Mbonge District Hospital were reviewed. The study population consisted of caregivers of children aged 9-23 months. All caregivers whose children had vaccination cards and caregivers whose children did not have vaccination cards but could recall the vaccines that the child had taken were enrolled into the study. This age group was chosen because a child is expected to finish his/her routine vaccines at the age of 9 months according to the Cameroon vaccination calendar and also for evaluations of routine vaccination coverage, target populations are defined in 12-month groups to represent the births in a one-year period.
2.2. Sample Size and sampling
A sample size of 296 study participants was calculated at a specified confidence interval of 95% and a precision or an acceptable error margin of 5% (0.05). This sample size was calculated using the formula by Brown et al.9 A vaccination coverage of 74% which is the overall vaccination coverage from a previous study carried out after the measles outbreak that occurred in Maroua, Cameroon in 20097 was used in sample size calculation. A sample size of 296 was the expected sample; however, a total of 300 study participants aged 9- 23 months were enrolled into the study.
2.3. Data collection
2.3.1. Administration of questionnaires to caregivers
Children aged 9-23 months were selected from the households through door to door visits. In cases where two or more 9-23 months old children lived in the same household, the youngest child was selected. Informed consent was obtained from caregivers through a signature of the informed consent form after adequately explaining the objectives and protocol of the study. A structured interviewer-administered questionnaire was used to obtain information from consenting parents and all participants were free to withdraw from the study at any time without any consequence. The questionnaire was formulated from a review of available literature on immunization surveys in developing countries.
The logical structure of the questionnaire was checked on the field, during a pre-testing carried out in Muea health area, specifically Muea village. In all, 15 questionnaires were administered during pre-testing and corrections were made. This questionnaire was used to collect information that identified the factors that influenced vaccination coverage levels in the Mbonge health area. Based on Parents’ recall or review of children’s vaccination cards aged 9-23 months, children were classified into three groups: (1) partially vaccinated, (2) fully vaccinated, and (3) not vaccinated at all. If a child was partially or not vaccinated at all, the caregiver was asked reasons why the child was not vaccinated. Missed vaccination dates were abstracted from the vaccination cards. Questionnaires were also used to assess parent’s knowledge on vaccination, these questionnaires were written in English but administered to participants in “pidgin English.” Questions include: what is the importance of vaccination, name some vaccines and diseases they prevent, etc. This knowledge was scored on the scale of 0-14, when a respondent scored below 4.6 it meant poor knowledge on vaccination, 4.7-9.3 meant average and above 9.4-14 meant good knowledge on vaccination.10 Utility of the health facility was assessed by asking questions related to distance to the health facility, if the mother attended antenatal care (ANC), if the nurses had explained to them what vaccination was all about, if they understood the vaccination calendar, if they understood the importance of vaccination and whether they benefited from outreach programs organized by health facilities.
2.3.2. Review of vaccination records
A retrospective study was done by reviewing vaccination records from the Mbonge District Hospital. Mbonge health area has a total of 6 health facilities two of which are non-functional. Mbonge District Hospital was chosen for its records to be reviewed because it covers 13 out of the 28 communities in the Mbonge health area, thus covering about three quarter of the total population of the health area. Vaccination records from 1 January 2014 to 31 December 2016 were reviewed. The data from these records provided information on the vaccination coverage for each vaccine, (under the expanded program on immunization) know the trend of vaccination coverage over the past 3 years, obtain information on measles vaccine coverage levels for the past 3 years and possible reasons for the reoccurrence of measles outbreak. The total number of children eligible for vaccination for each year was obtained from official census. This census data was used to calculate monthly and yearly targets for vaccination. Vaccination coverage over the years was obtained.
2.4. Data Management and Analysis
Data obtained by review of hospital records and questionnaire administration were entered in a template designed in Epi Data version 3.1. (Lauritsen JM & Bruus M. EpiData)11. A comprehensive tool for validated entry and documentation of data. The EpiData Association, Odense, Denmark, 2003-2005) The data were verified for completeness and consistency. It was cleaned and exported to SPSS v 20 (IBM Corp. Released 2011. IBM SPSS Statistics for Windows, Version 20.0. Armonk, NY: IBM Corp) for analysis. The data were secured in a password protected file in the investigator’s computer. Association between the dependent variable (vaccination status) and independent variable (educational level of caregivers, and distance to health facility and covariates such as religion, marital status and occupation) variables were computed by the chi-square test. Statistical significance of difference or associations was designated at P<0.05.
2.5. Ethical Considerations
Administrative and Ethical clearances were obtained from the Buea Regional Delegation of Public Health and the Faculty of Health Science Institutional Review Board, University Buea, respectively. Authorization was also obtained from the District Medical Officer (DMO) of the Mbonge Health District. An information sheet on the study was written in the simplest language possible for the participants to read and understand before they could make a decision to participate. Only mothers who granted informed consent and signed the consent form could participate in this study. For those who could not read a witness was there to read and explain to them to enable them make a decision. Each questionnaire was coded to ensure confidentiality, so that participant information could not be disclosed or understood by any other person apart from investigators who took part in the study. All respondents were free to withdraw from the study at any time along the study.
3. Results
3.1. Age, Sex and Characteristics of the Study Participants
A total of 300 caregivers responded to the questionnaires that were administered. Out of the 300 caregivers who participated in the study, 272 (90.7%) were mothers, 12 (4%) were fathers and 16 (5.3%) were other people. Majority (96%) of the caregivers was females; their mean age was 27 years (±6.864) ranging from 16 to 60 years with majority (50%) of the caregivers falling between the age groups of 16-25 years. Most (69.3%) of the care givers were farmers with majority (43%) attaining primary school education. Two hundred and eighteen (72.7%) of the caregivers were married and a majority (95.7%) of the caregivers were Christians (Table 1).
| Indicator | Categories | N (%) |
|---|---|---|
| Primary caregiver | Mother | 272 (90.7) |
| Father | 12 (4.0) | |
| other people | 16 (5.3) | |
| Age of caregiver (years) | 16-25 | 150 (50) |
| 26-35 | 116 (38.7) | |
| 36+ | 34 (11.3) | |
| Gender | Female | 288 (96.0) |
| Male | 12 (4.0) | |
| Occupation | Farming | 208 (69.3) |
| Business | 60 (20) | |
| Student | 32 (10.7) | |
| Educational level | Did not go to school | 16 (5.3) |
| Primary | 129 (43.0) | |
| Secondary | 133 (44.3) | |
| Tertiary | 22 (7.3) | |
| Marital status | Married | 218 (72.7) |
| Single | 72 (24.0) | |
| Divorced | 2 (0.7) | |
| Widow/ Widower | 8 (2.7) | |
| Number of children | 1-3 | 204 (68.0) |
| 4-8 | 96 (32.0) | |
| Religion | Christians | 287 (95.7) |
| Muslim | 2 (0.7) | |
| Ancestral/Traditional religion | 11 (3.7) | |
3.2. Description of the Children Enrolled into the Study
The vaccination coverage survey included 300 children. Females (52%) were slightly more than males (48%). The minimum age of the children was 9 months and maximum were 23 months. Most of the children (61.3%) were delivered in a health center; 36% of the children were delivered at home; and 2.7% were delivered in a village clinic. About sixty-nine point three per cent (69.3%) of the children had the BCG mark on their left arm. Among the 300 children involved in this study, 255 (85%) of them had vaccination cards while 45 (15%) did not have vaccination cards (Table 2).
| Indicator | Categories | N (%) |
|---|---|---|
| Gender | Female | 156 (52.0) |
| Male | 144 (48.0) | |
| Age | 9-23months | 300 (100) |
| Child’s birth place | Health center | 184 (61.3) |
| Village clinic | 8 (2.7) | |
| Home | 108 (36.0) | |
| Presence of BCG mark on child | Yes | 208 (69.3) |
| No | 92 (30.7) | |
| Availability of vaccination cards | Yes | 255 (85.0) |
| No | 45 (15.0) | |
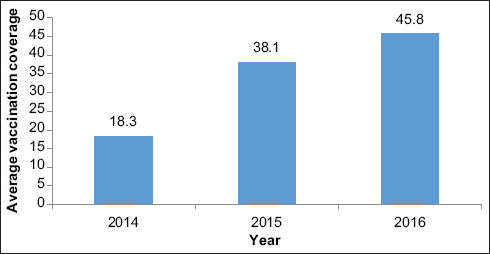
3.3. Vaccination Coverage Levels of all Vaccines from 2014 – 2016
The vaccination coverage levels for the past 3 years among the respondents have been improving. With the year 2014 having the lowest coverage levels (18.3%) and 2016 having the highest vaccination coverage levels (45.8%). This gave an average vaccination coverage of 34.0% over the past three years in the Mbonge Health Area (MHA). The vaccination coverage level of each vaccine has been increasing progressively over the years though at a very low rate. In 2014 measles had the lowest coverage of 2.6% and Oral poliovirus vaccines (OPV-1) having the highest with a coverage level of 57%. The rest of the vaccines did not attain a coverage level up to 60% (Figure 1).
- Trends in measles vaccination coverage rates from 2014-2016
3.4. Factors Affecting Vaccination Coverage Levels in the MHA
3.4.1. Demographic factors affecting vaccination of children in MHA
Some demographic factors that influenced vaccination coverage levels in Mbonge Health Area. Factors such as the type of care giver, age of care giver, gender of caregiver, educational level and religion showed no significant association (p-value>0.05) with the vaccination status of the study children. In contrast, occupation and marital status showed a significant association (p-value<0.05) with respect to vaccination status of children (Table 3).
| Indicators | Categories | Children status | Significance of difference | 95% CI | Total | |
|---|---|---|---|---|---|---|
| Completely vaccinated | Partially or not vaccinated at all | |||||
| Primary care giver | Mother | 130 (47.7%) | 142 (52.2%) | c2=5.077 P=0.079 | 0.218-7.462 | 272 |
| Father | 9 (69.2%) | 4 (30.8%) | 0.0303-108.44 | 13 | ||
| Other | 4 (26.7%) | 11 (73.3%) | 0 | 15 | ||
| Age of care giver | 16-25 | 65 (43.3%) | 85 (56.7%) | c2=3.079 P=0.215 | 0.191-2.291 | 150 |
| 26-35 | 58 (50%) | 58 (58%) | 0.238-2.323 | 116 | ||
| 36+ | 20 (58.8%) | 14 (41.2%) | 34 | |||
| Gender | Female | 137 (47.6%) | 151 (52.4%) | c2=0.027 p=0.550 | 0.184-27.16 | 288 |
| Male | 6 (50%) | 6 (50%) | 12 | |||
| Occupation | Farming | 92 (44.2%) | 116 (55.8%) | c2=14.96 P=0.011* | 0.29-0.788 | 208 |
| Business | 34 (56.7%) | 26 (43.3%) | 0.108-2.699 | 60 | ||
| Student | 17 (53.1%) | 15 (46.1%) | 32 | |||
| Educational level | Never been to school and primary | 63 (43.4%) | 82 (56.6%) | c2=2.002 P=0.097 | 0.692-2.957 | 145 |
| Secondary and tertiary | 75 (48.4%) | 155 | ||||
| Marital status | Married | 97 (44.5%) | 121 (55.5%) | c2=3.215 P=0.048* | 0.185-1.155 | 218 |
| Single home | 46 (56.1%) | 36 (43.9%) | 82 | |||
| Religion | Christians | 140 (48.8%) | 147 (51.2%) | c2=3.294 P=0.61 | 0.111-13.308 | 287 |
| Ancestral/traditional religion | 3 (23.7%) | 10 (76.9%) | 13 | |||
3.4.2. Knowledge of vaccination and its effect on vaccination coverage levels
Looking at the scores, 94.3% (283) of the participants had very poor knowledge on vaccination, 5.7% (17) had between 4.7-9.3, are classified as having average knowledge on vaccination while no one fell in the category 9.4-14, thus indicating that knowledge on vaccination was still not really adequate. The findings from this study showed that 128 (45.2%) children who were completely vaccinated were of parents who had poor knowledge on vaccination, while 15 (88.2%) completely vaccinated children were of parents who had an average knowledge on vaccination. There was a statistically significant association between knowledge on vaccination and vaccination status of the study children (P<0.05), suggesting that the better the knowledge the better the compliance to vaccination (Table 4).
| Category | N (%) | |
|---|---|---|
| Importance of vaccination | Yes | 291 (97) |
| No | 9 (3) | |
| If no why? | No reason | 6 (2) |
| does not see the need | 1 (0.3) | |
| her child is strong | 1 (0.3) | |
| Her children never get sick | 1 (0.3) | |
| Encouraging other women to Vaccinate their children | Yes | 286 (95.3) |
| No | 14 (4.7) | |
| Number of times polio vaccine should be given to child | 2 | 12 (4) |
| 4 | 48 (16) | |
| 6 | 16 (5.3) | |
| Don’t know | 224 (74.7) | |
| Age at which measles vaccine has to be take | 2months | 5 (1.7) |
| 7months | 16 (5.3) | |
| 9months | 127 (42.3) | |
| Others | 152 (50.7) | |
| Age at which vaccine should be completed | 5months | 5 (1.7) |
| 9months | 95 (31.7) | |
| 12months | 23 (7.7) | |
| Don’t know | 177 (59) | |
4. Discussion
An assessment of routine vaccination coverage, risk factors for incomplete vaccination and the association between vaccination coverage levels and reoccurrence of diseases like measles among children aged 9–23 months was conducted in the Mbonge Health Area, Kumba South Region, Cameroon. The study was done following a measles outbreak that occurred in the Mbonge health area specifically Big Nganjo in March 2016. Comparing the individual vaccine coverage levels obtained from the past three years to the WHO target (90%), it showed that no vaccine coverage had attained this target. Measles whose target towards elimination was 95% had 14.87% as average vaccine coverage over the past three years.
Among the caregivers interviewed, only 255 (85%) of the children had vaccination cards. According to their vaccination cards plus parent’s recall 47.7% (CI: 41.9-53.47) of the children in this survey were fully vaccinated. This result is high when compared with the vaccination coverage rates reported from surveys in other rural African areas which ranged from as low as 26% in Burkina Faso12 to 88% in Ghana.13 Compared with a similar study in Dschang, West Region of Cameroon following the polio outbreak in 20136 a high vaccination coverage level of 85.9% was attained which was far higher than the 47.7% coverage that was recorded in this study. This difference may be due to differences in geographical area location, living standards and level of education of the people that influenced the knowledge on vaccination hence vaccine compliance rate. In this study 10% of the children were not vaccinated at all. This observation is higher compared with the 2.6% reported by the 2011 Demographic Health Survey (DHS) for the West region of Cameroon. Several factors were associated with the incomplete vaccination status of children but only six of them were statistically significant.
The percentage of children completely vaccinated among business owners were higher (56.7%) than the percentage for farmers (44.2%). This is in line with a similar study carried in Jimma town South West Ethiopia.14 This may be because farming was the main occupation of people in the rural areas. Since it was their main source of income, they dedicated a lot of attention and investments on their farms so as to get the best products for sale to generate income. Most people who were married were more likely to have completed their children’s vaccines than single parents. This observation is in contrast with a study carried out in the Sianana District Southeast Ethiopia10 where the marital status of caregivers did not have a significant effect on the vaccination status of the children. This maybe because most married mothers received support from their husbands to take the children for vaccination while single parents do not receive this kind of support.
In this study, educational level (primary, secondary, tertiary and illiterates) of caregivers was not among the determinants of vaccination completion. This finding is non-consistent with the findings from a study carried out in Sianana District Southeast Ethiopia,10 which showed that caregivers who attended secondary and above level were two times more likely to complete the vaccination of their children than caregivers who did not go to school. Other factors like primary care giver, religion, gender and age of care givers did not show a significant association with the vaccination status of the children from this health area.
Non-Utilization of health facilities and ANC attendance during pregnancy was associated with the partial or not being vaccinated at all status of the children. This is in line with studies from other African countries such as Ghana.13 This observation may due to the fact that limited contact with health facilities especially during pregnancy may lead to less information on vaccination. This study also showed that utilization of health care facilities was associated with children’s vaccine completion. This finding is in line with a study carried out in Ethiopia15 which reported that children’s whose mothers used health facilities and attended ANC were more likely to be fully vaccinated. This could be due to mother’s health seeking behavior during which they may discuss with health professionals on vaccines and vaccine preventable diseases, its importance, time of vaccine initiation, completion and possible side effects associated with vaccine during follow up. This information may have motivated mothers to get their children vaccinated and also motivate other mothers to use health facility services. Distance to the health facilities did not have any significant difference when it came to vaccination status of children which was not the case with a study carried out in Mozambique,16 which reported that distance to the health facilities hindered the completion of vaccination of children. The services of health facilities were graded. This study showed that there was a significant association between the grades of the services offered by health facilities and the vaccination status of the children. Among those who graded the services of the health facility as good, 58.6% of their children were completely vaccinated.
Findings from this study showed that knowledge of caregivers on vaccination had a great influence on the vaccination status of a child; a high knowledge on vaccination was associated with the complete vaccination status and vice versa. In this study no study participant had a high score on the vaccination knowledge. Rather children whose caregivers had an average or sufficient knowledge on vaccination were twice more likely to be completely vaccinated than those whose mothers had low knowledge. This is in line with a study carried out in Nigeria.17 As knowledge of care givers on vaccination is improved, they develop a positive attitude towards vaccination then they could be motivated to complete the child’s vaccinations.
Routine vaccination and active disease surveillance have been shown to adequately decrease frequency and severity of outbreaks. The recent measles outbreak in Big Nganjo a community in Mbonge health area confirms that there exist some flaws in policies aimed at controlling measles spread in Cameroon. A highly immunized population can limit the spread of measles18. The reason for this outbreak that occurred in Mbonge health area in 2016 was probably because of poor measles vaccination coverage which is consistent with the cause of the measles outbreak that occurred in Misaje, North West region of Cameroon in 2008.7 This is also similar to the cause of the measles epidemic that occurred in Maroua, Cameroon 2008-2009 which showed that measles incidence was inversely proportional to routine vaccination coverage.8
4.1. Limitations
Difficulties in the accessability of the study area, telephone network challenges during the study period. There is also a limitation of recall bias as parents and caregivers may not remember whether their children completed their vaccinations, or in some cases the kinds of vaccines that were administered.
4.2. Recommendation for Further Studies
Targeting younger parents and families living far from health or vaccination centres with appropriate immunization promotion strategies, and the improvement of prenatal care and delivery services should be addressed in order to increase vaccination coverage and timely vaccine administration. Information and attitudes towards immunisation should be strengthened with adequate vaccination education programs. Increased enrolment of girls into secondary school should be generally encouraged and is likely to have a favourable impact on vaccination rates of their future offspring. ontinuous education of women at the health facilities would lead to an increase in the approval or acceptance for vaccination. Furthermore, parents’ poor support for immunization services as a result of the quality of care provided has implications and deserves consideration for routine immunization program. New immunization strategies should be adopted in this area ensuring that every child weather born at home or health facility should be completely vaccinated.
5. Conclusion and Global Health Implications
This study revealed a low vaccination coverage rate of 34.0% in the Mbonge Health Area (South West region, Cameroon). Factors such as low knowledge on vaccination, being a farmer, being married, caregiver’s non-utilization of health services, good services provided by health facilities and attending ANC during pregnancy were found to affect the vaccination status of the children hence vaccination coverage levels in the Mbonge Health Area. It was found out that the main reason for measles reoccurrence in this health area was the incompleteness in the vaccination status of children in the locality which was mainly due to high dropout rates.
Acknowledgements:
The authors are grateful to the caregivers of the children who took part in this study.
Competing interests: The authors declare that they have no conflict of interest.
Financial Disclosure: None.
Funding/Support: None.
Ethics approval: Ethical approval was granted by the Institutional Review Board of the Faculty of Health Sciences of the University of Buea. Administrative approval was obtained from the Director of the Bamenda Regional Hospital.
References
- Immunizing school-age children and adolescents:experience from low-and middle-income countries. Vaccine. 2010;28(5):1138-47.
- [Google Scholar]
- Vaccine Hesitancy:A Growing Concern. Paediatr Drugs. 2020;22(2):105-111. doi:10.1007/s40272-020-00385-4
- [Google Scholar]
- Making markets for vaccines. In: Report of the Center for Global Development. 2005.
- [Google Scholar]
- Disease Control Priorities in Developing Countries (2nd edition). Washington, DC: The International Bank for Reconstruction and Development, The World Bank; 2006.
- Vaccine coverage and determinants of incomplete vaccination in children aged 12–23 months in Dschang, West Region, Cameroon:a cross-sectional survey during a polio outbreak. BMC Public Health. 2015;15:630. https://doi.org/10.1186/s12889-015-2000-2
- [Google Scholar]
- A long-lasting measles epidemic in Maroua, Cameroon 2008-2009:mass vaccination as response to the epidemic. J Infect Dis. 2011;204(Suppl 1 (Suppl 1)):S243-S251. doi:10.1093/infdis/jir093
- [Google Scholar]
- Measles outbreak in a poorly vaccinated region in Cameroon:a case series study, public health challenges and recommendations:Global Polio Eradication Initiative Polio this week. Wild_poliovirus_list_ 2010-2015. Pan African Medical Journal. 2015;22:163.
- [Google Scholar]
- An assessment of child immunization coverage and its determinants in Sinana District, Southeast Ethiopia 2015. BMC Pediatrics. 2015;15:31.
- [Google Scholar]
- A comprehensive tool for validated entry and documentation of data 2003. The EpiData Association, Odense Denmark
- [Google Scholar]
- Assessment of factors associated with complete immunization coverage in children aged 12-23 months:a cross-sectional study in Nouna district, Burkina Faso. BMC Int Health Hum Rights. 2009;9(Suppl 1(Suppl 1)):S10. doi:10.1186/1472-698X-9-S1-S10
- [Google Scholar]
- Immunization coverage in an under-served Peri-urban community in Ghana 2014. International Journal Maternal Child Health. 2014;2:32-38.
- [Google Scholar]
- Reasons for defaulting from the Expanded program of immunization in Jimma town south western Ethiopia. Ethiopia Journal of Health Science. 1999;9:93-100.
- [Google Scholar]
- An assessment of child immunization coverage and its determinants in Sinana District, Southeast Ethiopia. BMC Pediatr. 2015;15(31) https://doi.org/10.1186/s12887-015-0345-4
- [Google Scholar]
- Assessing immunization data quality from routine reports in Mozambique. BMC Public Health. 2005;5:108. https://doi.org/10.1186/1471-2458-5-108
- [Google Scholar]
- Factors predicting BCG immunization status in northern Nigeria:a behavioral-ecological perspective. J Child Health Care. 2009;13(1):46-62. doi:10.1177/1367493508098380
- [Google Scholar]
- International measles incidence and immunization coverage. J Infect Dis. 2011;204(Suppl 1):S158-S163. doi:10.1093/infdis/jir124
- [Google Scholar]



